Brief Summary
Jurdan MENDIGUCHIA, Adrian CASTAÑO-ZAMBUDIO, Pedro JIMENEZ-REYES, Jean–Benoît MORIN, Pascal EDOUARD, Filipe CONCEIÇÃO, Jonas DODOO, Steffi L. COLYER
https://journals.humankinetics.com/view/journals/ijspp/17/3/article-p374.xml
Hamstring strain injuries (HSIs) continue to be highly prevalent and impose a substantial burden in sports characterised by high-speed running. Although eccentric-focused strength training has consistently been proposed as an effective preventive measure, the incidence of HSIs has not decreased over the past 40 years. The following summarises work by Mendiguchia and his ongoing investigation into the relationship between anterior pelvic tilt (APT) and HSI.
Unlike other pathologies, such as anterior cruciate ligament injuries or groin pain, there have been no studies that have biomechanically corrected the primary injury mechanism of HSIs. Consequently, it is imperative to investigate variables beyond eccentric strength, including sprinting mechanics, which may influence the injury mechanism. Anterior pelvic tilt (APT) has been reported to be closely associated with instances when the hamstring muscle-tendon tissues experience the highest mechanical strain during sprinting. Theoretically, an increased APT would cause a superior translation of the ischial tuberosity, resulting in greater active lengthening and passive tension demand on the posterior thigh musculature due to an increased moment arm derived from the relative hip flexion generated.
Therefore, the aim of this study was to investigate whether a specific 6-week multimodal intervention, combined with an on-field running technique program, would induce changes in pelvis and lower limb kinematics at maximal speed. Based on the recent study by Mendiguchia et al (2020) which demonstrated changes in APT during gait locomotion, it was hypothesised that the multimodal training program (involving lumbopelvic control exercises and sprint technique training) proposed in this pilot study would lead to a decrease in APT, along with alterations in other biomechanical variables during the maximum running speed phase of the sprint. These changes are expected to align with a more front-side oriented sprint technical model, characterised by a more upright trunk position, a higher maximum vertical knee position during the swing phase, a reduced distance between the knees, and a shorter touchdown distance at initial contact.
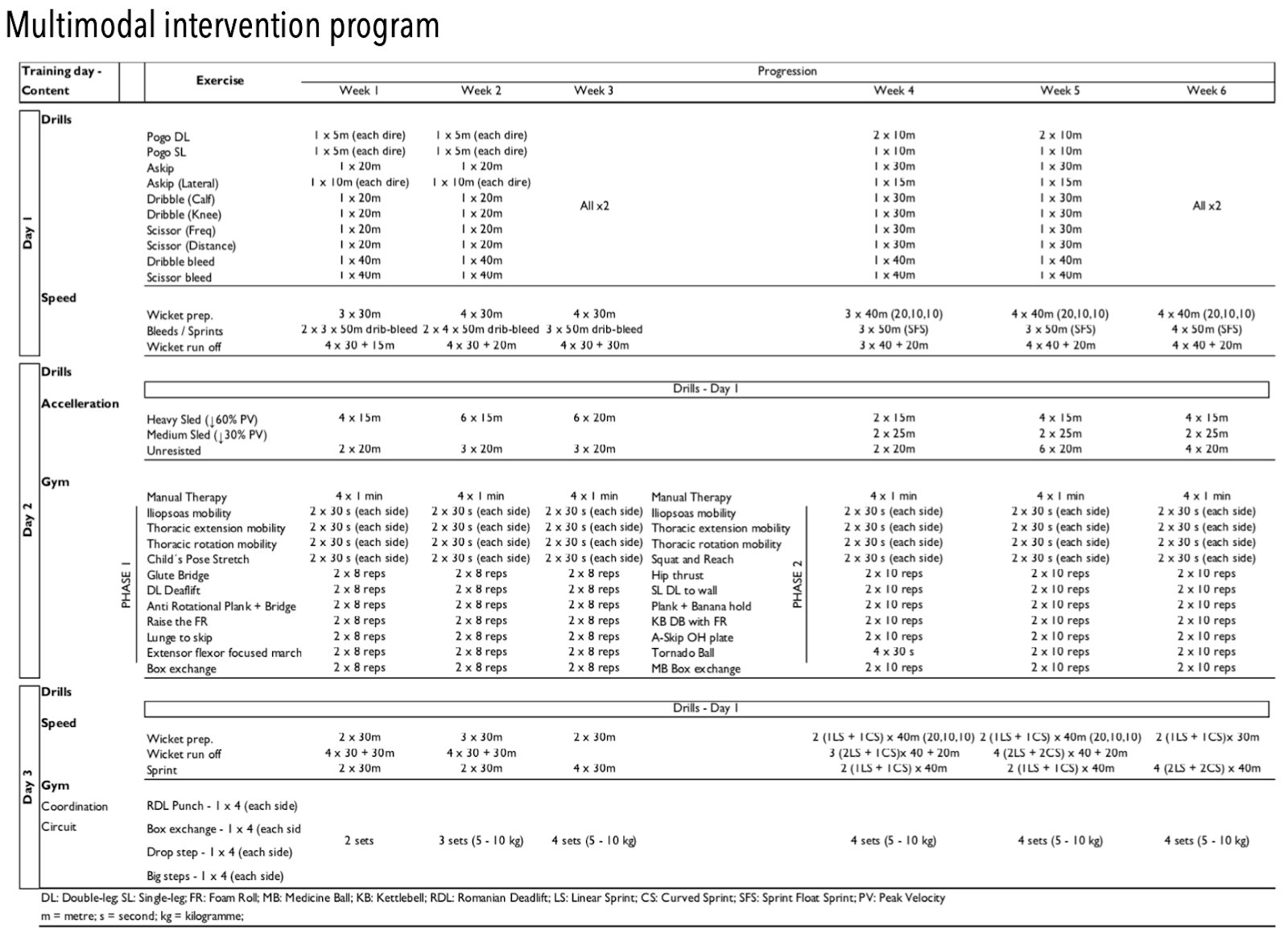
A comparative trial with testing sessions split by a 6 week time span where an exercise intervention program was conducted. Fifteen amateur male athletes were separated into control (8 athletes) and intervention (7 athletes) groups. For testing, following a warm up, athletes were asked to maximally sprint twice for 35 meters while kinematic and max speed data was recorded. Using 24 surface markers and a 15 camera motion analysis setup, seven key events were identified and analysed during each stride cycle; toe-off (TO), maximal hip extension (MHE), maximal vertical knee displacement (MVKD), maximal vertical projection (MVP), maximal hip flexion (MHF), touchdown (TD) and full support (FS). During the captured stride cycles, relevant dependent variables for ipsi- and contralateral leg were selected for the subsequent analysis such as joint angles or segment orientations. Athletes in the intervention group participated in a multimodal training program consisting of 3 sessions per week over a 6-week period. The training program encompassed coaching, strength and conditioning, and physical therapy components. During the intervention, athletes were prohibited from continuing their usual training routines.
Results
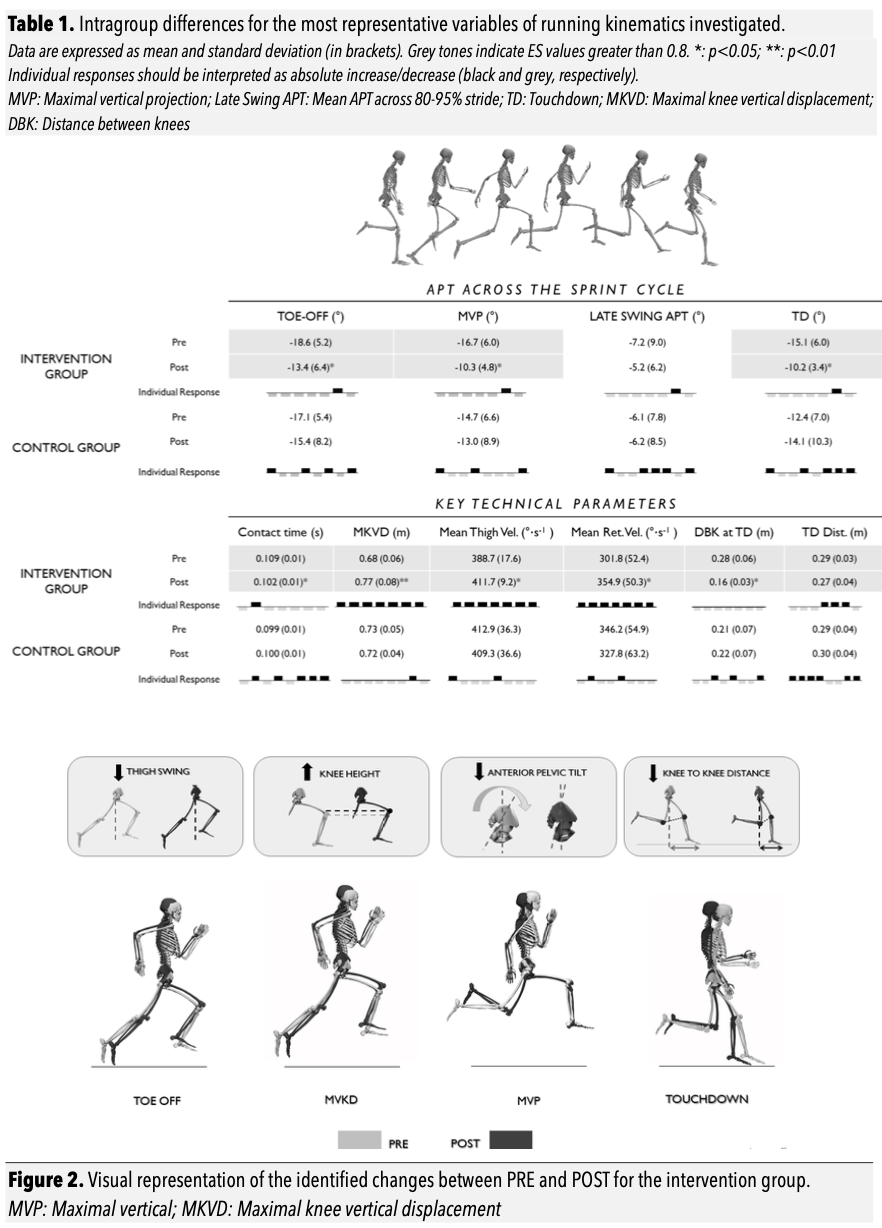
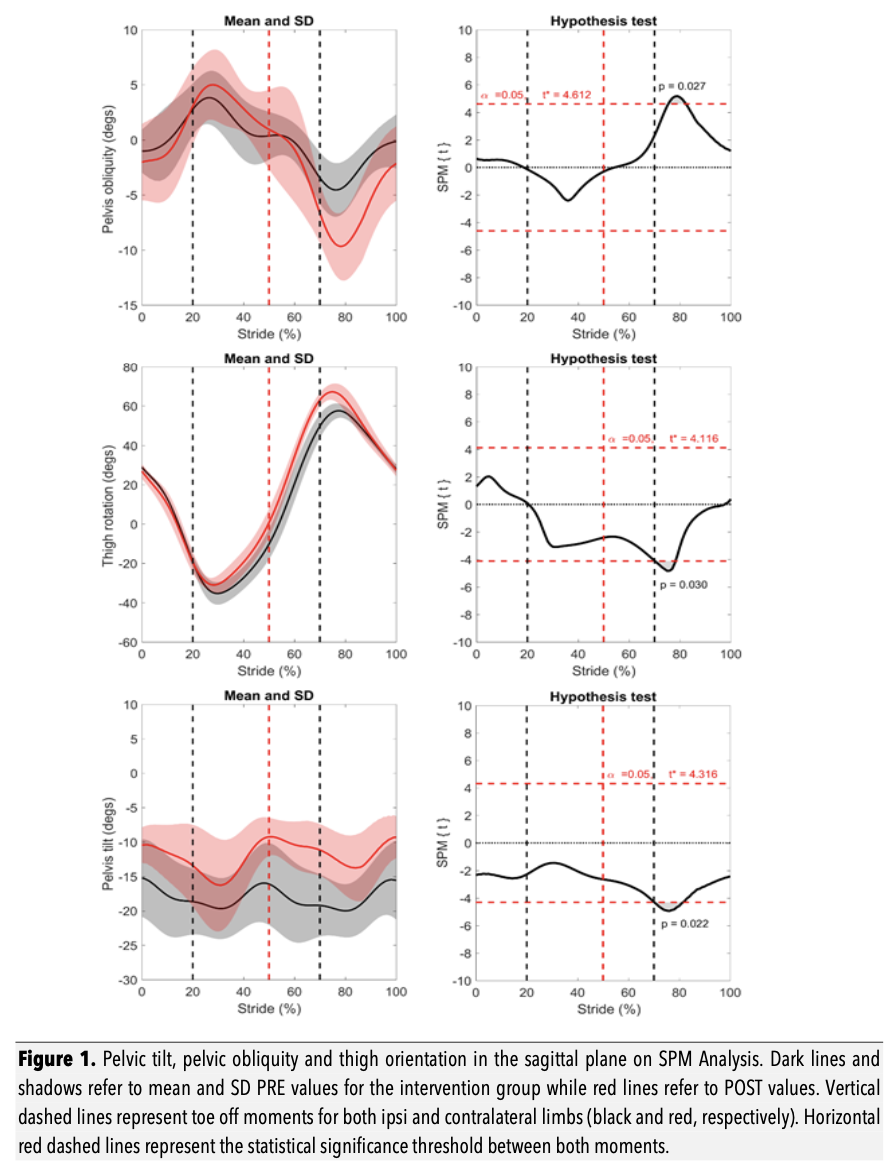
No significant differences were found between groups during initial testing when analysing segment and joint curves using SPM or independent t-tests. After the 6-week period, post intervention testing analysis revealed differences in the pelvic and thigh segments in the sagittal plane for the IG (Figure 1), but not for the CG. Further discrete analysis of these variables identified numerous significant differences in joint angles and segment orientations at defined key moments. The most representative variable differences are summarised in Table 1 and visually illustrated in Figure 2.
Discussion
The main findings of the study validate the authors' initial hypothesis that a 6-week multimodal intervention, combining lumbopelvic control exercises with a running technique program, induced significant changes in sagittal and frontal plane kinematics of the pelvis at maximal speed. This intervention resulted in a lower anterior pelvic tilt (APT) during the late swing phase and a higher pelvic obliquity on the free leg side during the early swing phase. Additionally, the kinematics of the lower extremities were modified according to front-side mechanics principles, leading to an increase in the maximum knee height, an increase in thigh angular retraction velocity, a decrease in the distance between the knees (DBK) at initial contact, a shorter landing distance, and reduced contact time. These modifications were accompanied by improved sprint performance, as evidenced by significant decreases in the 0-5, 5-10, 10-15, and 25-35 meter split times, as well as the 0-20 and 0-35 meter cumulative split times during the maximum sprint test, compared to the control group over the same period.
One reason for the higher prevalence of biceps femoris injuries may be related, among other factors, to a greater non-uniform elongation peak of the proximal biceps femoris during the late swing phase of maximal speed sprinting. Given that strain is a major determinant of tissue failure, and considering that the ipsilateral elongation peak of the biceps femoris coincides with the contralateral iliacus maximum stretch and the second peak of pelvic anterior tilt during the late swing phase, it seems logical to expect that a posterior tilt of the pelvis, as observed in this study, would reduce the suggested stretch and eccentric demand on the biceps femoris musculotendon, particularly in its proximal region.
In conclusion, the incorporation of lumbopelvic control exercises alongside a running technique program resulted in reduced anterior pelvic tilt (APT). This combined intervention can be viewed as an additional component within a multifaceted rehabilitation or prevention strategy, particularly beneficial for athletes exhibiting excessive APT and heightened susceptibility to hamstring strain injuries (HSI). To find out how KT360 can be utilised within a prevention strategy or rehabilitation to screen, monitor or train lumbopelvic complex please contact support@kangatech.com